
En este artículo publicado en Environmental Research, los autores abogan claramente por cambiar la consideración de la radiofrecuencia de posible cancerígeno a cancerígeno seguro. Para ello revisan varios de los artículos más relevantes publicados desde que, en 2011, la IARC catalogara esas emisiones como posible cancerígeno.
Estudios caso-control: glioma
La investigación de Aydin et al. (2011) realizada en niños con tumores cerebrales entre 2004 y 2008 en Noruega, Suecia, Dinamarca y Suiza, en niños y adolescentes entre 7 y 19 años, arroja resultados poco claros. Aunque las conclusiones reportadas no relacionaron el riesgo de tumor con el uso del teléfono móvil, un visionado más detallado de los resultados puede ofrecer interpretaciones diferentes (ver tabla).
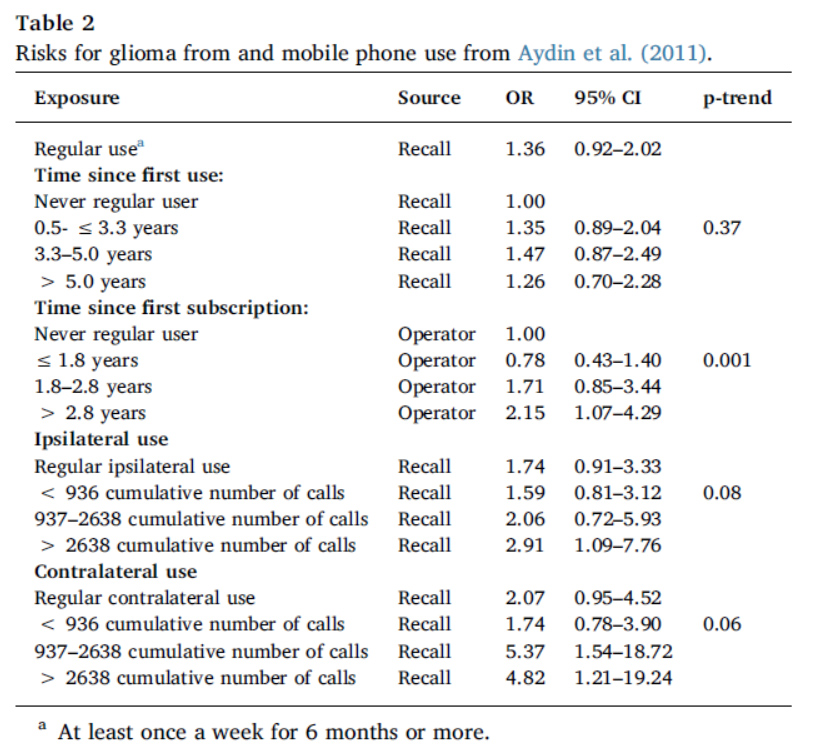
Como indican los autores, cuando se tomaron los datos del operador (y no los propiamente dados por los participantes) se aprecia un patrón significativo de respuesta a la dosis. Además, la tendencia encontrada en la respuesta a la dosis de exposición ipsilateral y contralateral, también bordea la significación al 95% (y recordemos que ese 95% no es ningún valor sagrado). Por tanto, mirando los datos en su totalidad, se podrían interpretar de manera diferente, y hay razones para considerar que puede haber una asociación.
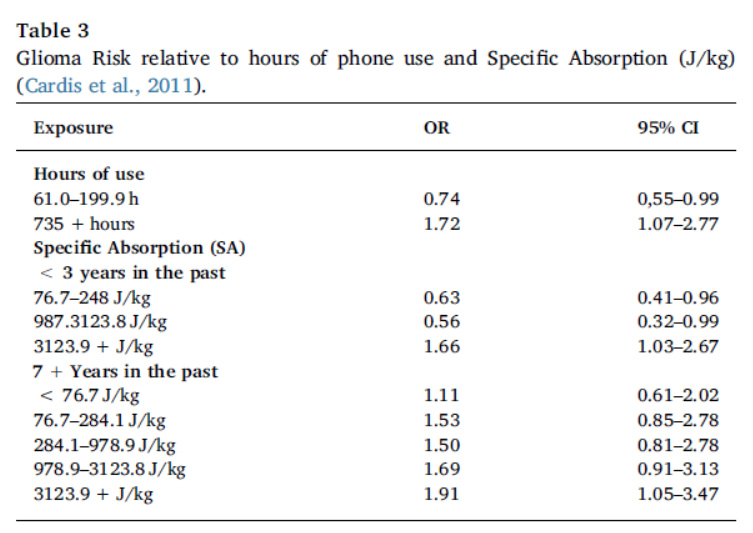
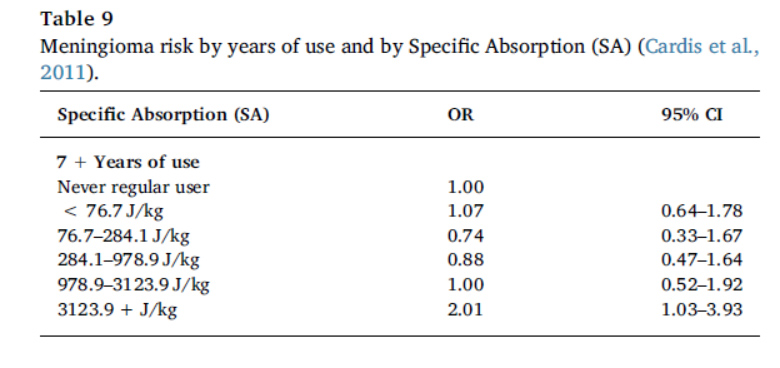
El estudio de Cardis et al. (2011), también arroja una respuesta a la dosis significativa, en esta ocasión considerando la dosis como radiación absorbida, y la respuesta como el riesgo de glioma y meningioma en 5 países (Australia, Canadá, Francia, Israel y Nueva Zelanda). La siguiente tabla muestra un resumen de los resultados.
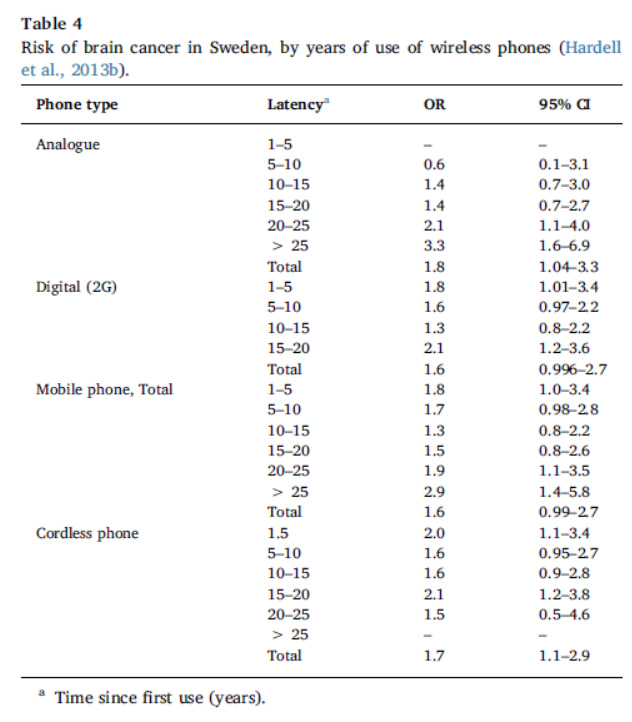
Hardell et al. (2013b), por su parte, en su estudio sobre cánceres cerebrales en Suecia entre 2007 y 2009, muestra también resultados significativos en función del tiempo de uso (ver tabla).
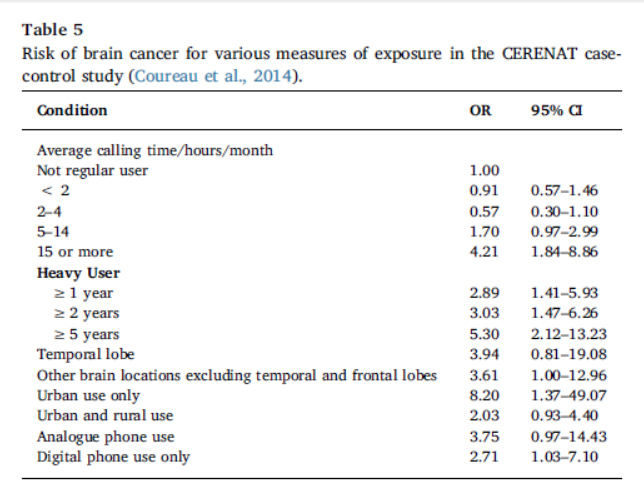
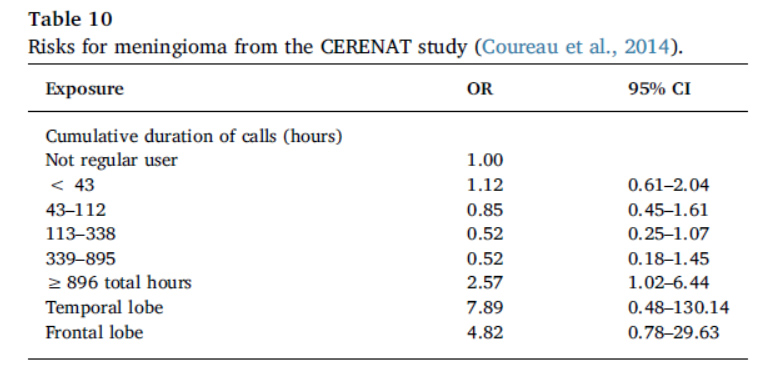
El estudio de Coureau et al. (2014), realizado en Francia entre 2004 y 2006 en personas con tumores cerebrales, de nuevo muestra un mayor riesgo con el incremento de tiempo de exposición (ver tabla).
Las investigaciones de Hardell & Carlberg (2015) y de Akhavan-Sigari et al. (2014) también muestran resultados a favor de la relación causal, mientras que Grell et al. (2016) y Momoli et al. (2017) re analizaron datos del estudio INTERPHONE, y encontraron que el riesgo de glioma se incrementaba con una mayor exposición., y que cambios genéticos asociados a efectos cancerígenos (mutación de la proteína supresora de tumores p53) se ligaban también a un mayor uso.
Estudios caso-control: meningioma
Los estudios de Cardis et al. (2011) y Couerau et al. (2014) encontraron sólo un incremento de riesgo significativo para usuarios con alta exposición (ver tablas siguientes).
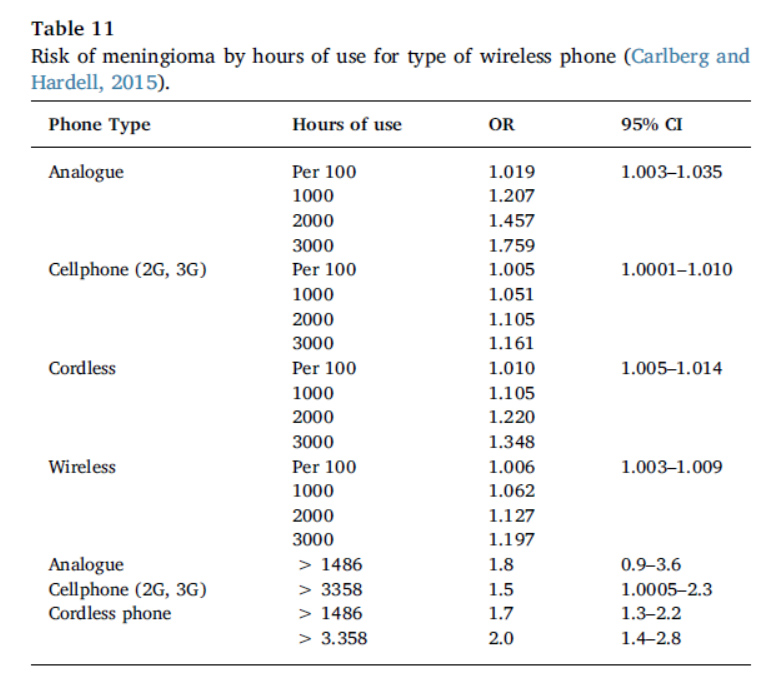
 Carbelg et al. (2013) no encontraron asociaciones significativas, pero Carlberg & Hardell (2015), en su estudio agregados entre los años 1997-2003 y 2007-2009, de nuevo encontraron un mayor riesgo para altas exposiciones (ver tabla).
Carbelg et al. (2013) no encontraron asociaciones significativas, pero Carlberg & Hardell (2015), en su estudio agregados entre los años 1997-2003 y 2007-2009, de nuevo encontraron un mayor riesgo para altas exposiciones (ver tabla).
Estudios caso-control de otros tipos de tumores
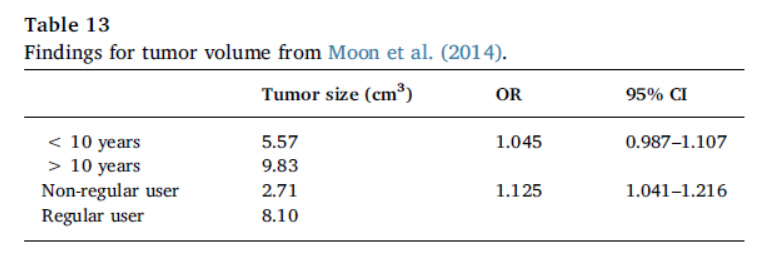
Destacan los estudios sobre Schwannoma vestibular de Moon et al. (2014) y Petterson et al. (2014) donde, en el caso del estudio de Moon et al. (2014) se encontró que los tumores tenían mayor volumen en función del tiempo de exposición y del uso del teléfono móvil.
Estudios de cohortes
La investigación de Frei et al. (2011) con un seguimiento de casi medio millón de personas durante más de una década no encontró asociación con el uso del teléfono móvil en cuanto a la incidencia glioma y meningioma. Este resultado, bastante relevante, sin embargo está sujeto a las críticas que los autores identifican: los usuarios que más habían empleado el teléfono móvil estaban considerados en el grupo de no expuestos, y aquellos que empezaron a usar el teléfono después de que la primera cohorte fuera establecida también se incluyeron en la categoría de no expuestos.
Sin embargo, el estudio de Benson et al. (2013), pese a realizar una medida limitada de la exposición al móvil no reportaron un incremento de riesgo de glioma, pero sí de Schwannoma vestibular. Ese estudio se realizó sobre un millón de mujeres en el Reino Unido.
Incidencia de tumores cerebrales
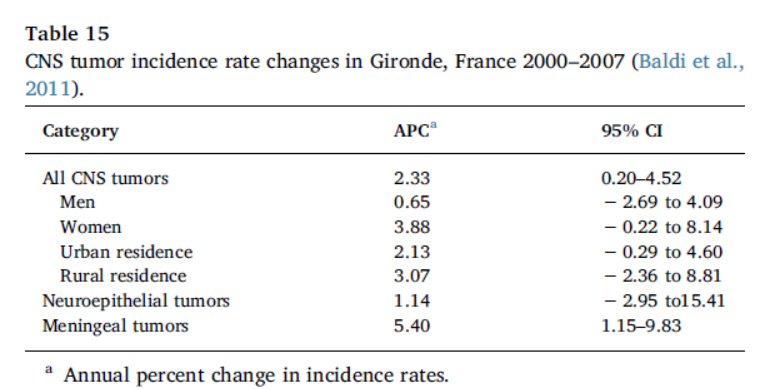
Los autores comentan varios estudios que han encontrado incrementos significativos de incidencia de tumores cerebrales. Por ejemplo, Baldi et al. (2011) en el periodo 2000-2007 encontraron una creciente incidencia de meningiomas (ver tabla), y globalmente también en el sistema nervioso central.
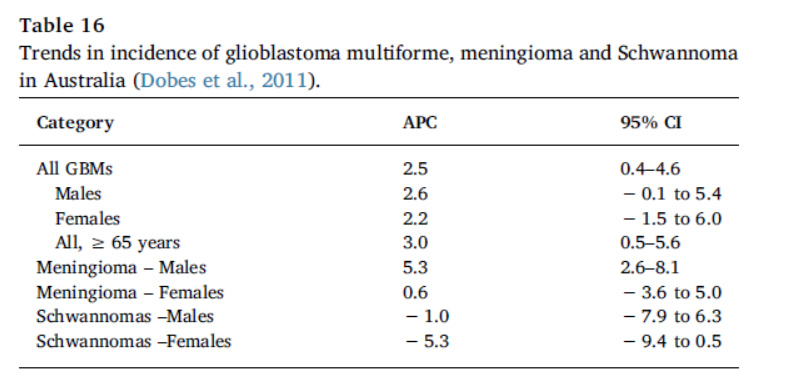 Dobes et al. (2011), en el periodo 2000-2008 en Australia, encontraron una mayor incidencia de gliobastoma multiforme, y también en meningiomas en hombres, aunque una menor incidencia de Schwannomas (ver tabla).
Dobes et al. (2011), en el periodo 2000-2008 en Australia, encontraron una mayor incidencia de gliobastoma multiforme, y también en meningiomas en hombres, aunque una menor incidencia de Schwannomas (ver tabla).
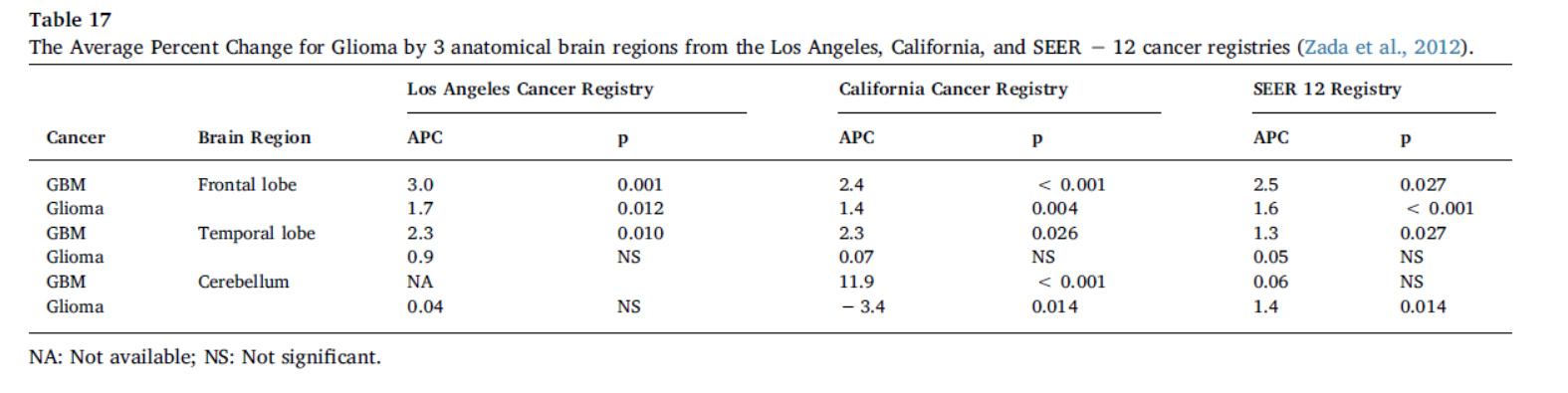
Zada et al. (2012), por su parte, examinaron datos de 3 registros de cáncer en Estados Unidos, encontrando incrementos en el glioma y el gliobastoma multiforme (ver tabla).
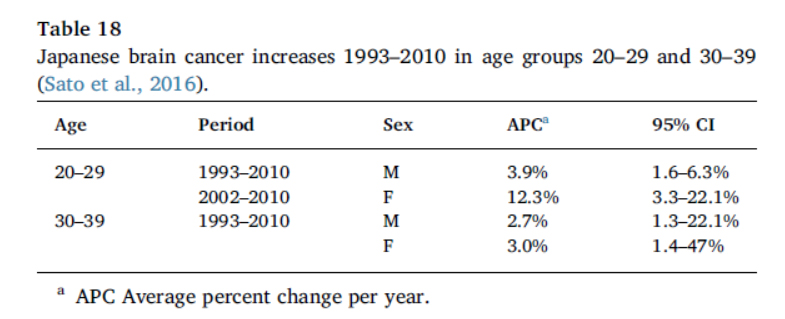
Sato et al. (2016) examinaron la incidencia de cáncer de cerebro en Japón, y los resultados mostraron un crecimiento significativo en los grupos de edad entre 20-29 y 30-39 años, durante el periodo 1993-2010 (ver tabla).
Series de casos
De interés también es el estudio de West et al. (2013) sobre casos de mujeres jóvenes que llevaban el teléfono móvil en sus sujetadores y desarrollaron cáncer de mama (ver tabla).

Los estudios de Peleg et al. (2012) y Peleg et al. (2018) sobre clusters de cáncer en trabajadores jóvenes de instalaciones de telecomunicaciones, y el estudio de Stein et al. (2011) sobre personal militar mostraron asimismo incidencias de cáncer por encima de lo esperado.
Comentarios
Como bien indican los autores, tanto los estudios caso-control como los de cohortes tienen limitaciones, pero esos posibles sesgos (sobre todo el de mala clasificación) tienden a favorecer la hipótesis nula (no efecto). No obstante, y teniendo en cuenta además de que 3 metanálisis recientes han encontrado un incremento significativo de riesgo de glioma en personas que han usado el móvil 10 o más años (Bortkiewicz et al., 2017; Prasad et al., 2017; Yang et al., 2017), los resultados (tomados con una perspectiva global) están más cerca del cancerígeno seguro que del posible cancerígeno.
Esto es lo que defienden los autores de este artículo, y abogan porque la IARC tan rápido como sea posible, tenga en cuenta esta evidencia y pase a catalogar la radiofrecuencia como cancerígeno tipo 1. Obviamente, esta evidencia debe contemplarse en conjunción con los estudios experimentales en animales, en especial los recientes resultados encontrados por el Instituto Ramazzini y el Programa Nacional de Toxicología de Estados Unidos.
Los autores defienden la aplicación del principio de precaución, y también el disfrute de la tecnología inalámbrica pero con una adecuada labor educativa sobre los riesgos que conlleva, así como una mejor y más adecuada regulación.
Además, el cáncer no es el único efecto negativo que este tipo de radiación puede causar, sino que la elecrohipersensibilidad, la disminución de la calidad del esperma o la pérdida de audición están también reportadas en la investigación. Esto, por sí solo, ya debería suponer una alerta pública sobre los perjuicios de usar indebidamente esta tecnología.
Bajo mi punto de vista, los estudios epidemiológicos mostrados indican globalmente un mayor riesgo de cáncer cerebral para usos prolongados y altos del teléfono móvil, lo que es en sí importante, pero que quizá podría llevar a una percepción inadecuada del riesgo. Los datos de esos estudios están en su mayor parte obtenidos hace varios años, cuando el despliegue y el uso de la tecnología inalámbrica era mucho menor. Por tanto, habría que preguntarse qué sucedería en usuarios moderados de teléfono móvil (referidos a las llamadas) pero que tienen un uso muy activo de la conexión inalámbrica.
Asimismo, y como también indican los autores, las poblaciones más vulnerables deberían de ser especialmente cautas, y los sistemas de salud pública establecer acciones para protegerlas. Reducir la exposición de los niños, tanto en casa como en los centros educativos es esencial.
Finalmente, y aunque no es habitual en las revisiones de artículos que hago en esta web, pongo a continuación todas las referencias del estudio, porque en este caso, lo creo fundamental para su entendimiento y para ampliar información.
Adams, J.A., et al., 2014. Effect of mobile telephones on sperm quality: a systematic review and meta-analysis. Environ. Int. 70, 106–112.
Akhavan-Sigari, R., et al., 2014. Connection between cell phone use, p53 gene expression in different zones of glioblastoma multiforme and survival prognoses. Rare Tumors 6 (3), 5350.
Aydin, D., et al., 2011. Mobile phone use and brain tumors in children and adolescents: a multicenter case-control study. J. Natl. Cancer Inst. 103 (16), 1264–1276.
Baldi, I., et al., 2011. Descriptive epidemiology of CNS tumors in France: results from the Gironde Registry for the period 2000–2007. Neuro-Oncol. 13 (12), 1370–1378.
Bandara, P., 2016. Mobile phone use and the brain cancer incidence rate in Australia. Cancer Epidemiol. 44, 110–111.
Belpomme, D., Campagnac, C., Irigaray, P., 2015. Reliable disease biomarkers characterizing and identifying electrohypersensitivity and multiple chemical sensitivity as two etiopathogenic aspects of a unique pathological disorder. Rev. Environ. Health 30 (4), 251–271.
Belpomme, D., Campagnac, C., Irigaray, P., 2016. Corrigendum to: reliable disease biomarkers characterizing and identifying electrohypersensitivity and multiple chemical sensitivity as two etiopathogenic aspects of a unique pathological disorder. Rev. Environ. Health.
Belyaev, I.Y., et al., 2009. Microwaves from UMTS/GSM mobile phones induce longlasting inhibition of 53BP1/-H2AX DNA repair foci in human lymphocytes. Bioelectromagnetics 30, 129–141.
Belyaev, I., 2010. Dependence of non–thermal biological effects of microwaves on physical and biological variables: implications for reproducibility and safety standards. In: Giuliani, L., Soffritti, M. (Eds.), European J. Oncol.—Library Non–Thermal Effects and Mechanisms of Interaction between Electromagnetic Fields and Living Matter, 5.
Ramazzini Institute, Bologna, Italy, pp. 187–218 (An ICEMS Monograph). Benson, V.S., et al. for the Million Women Study Collaborators, 2013. Mobile phone use and risk of brain neoplasms and other cancers: prospective study. Int. J. Epidemiol, vol. 42, pp. 792–802.
Bortkiewicz, A., Gadzicka, E., Szymczak, W., 2017. Mobile phone use and risk for intracranial tumors and salivary gland tumors – a meta-analysis. Int. J. Occup. Med. Environ. Health 30 (1), 27–43.
Cardis, E., et al., 2011. Risk of brain tumours in relation to estimated RF dose from mobile phones: results from five Interphone countries. Occup. Environ. Med. 68 (9), 631–640.
Carlberg, M., Hardell, L., 2012. On the association between glioma, wireless phones, heredity and ionising radiation. Pathophysiology 19 (4), 243–252.
Carlberg, M., Hardell, L., 2013. Use of mobile and cordless phones and survival of patients with glioma. Neuroepidemiology 40 (2), 101–108.
Carlberg, M., Hardell, L., 2015. Pooled analysis of Swedish case-control studies during 1997–2003 and 2007–2009 on meningioma risk associated with the use of mobile and cordless phones. Oncol. Rep. 33 (6), 3093–3098.
Carlberg, M., Söderqvist, F., Mild, Kjell H., Hardell, L., 2013. Meningioma patients diagnosed 2007–2009 and the association with use of mobile and cordless phones: a case-control study. Environ. Health 12 (1), 60.
Chapman, S., Azizi, L., Luo, Q., Sitas, F., 2016a. Has the incidence of brain cancer risen in Australia since the introduction of mobile phones 29 years ago? Cancer Epidemiol. 42, 199–205.
Chapman, S., Azizi, L., Luo, Q., Sitas, F., 2016b. Response from the authors to correspondence related to ‘Has the incidence of brain cancer risen in Australia since the introduction of mobile phones 29 years ago?’. Cancer Epidemiol. 44, 138–140.
Coureau, G., et al., 2014. Mobile phone use and brain tumours in the CERENAT case-control study. Occup. Environ. Med 71 (7), 514–522.
Degrave, E., et al., 2009. Causes of death among Belgian professional military radar operators: A 37-year retrospective cohort study. Int. J. Cancer 124, 945–951.
de Vocht, F., 2016. Inferring the 1985–2014 impact of mobile phone use on selected brain cancer subtypes using Bayesian structural time series and synthetic controls. Environ. Int. 97, 100–107.
Ding, L.X., Wang, Y.X., 2011. Increasing incidence of brain and nervous tumours in urban Shanghai, China, 1983–2007. Asian Pac. J. Cancer Prev. 12 (12), 3319–3322.
Dobes, M., et al., 2011. Increasing incidence of glioblastoma multiforme and meningioma, and decreasing incidence of Schwannoma (2000–2008): findings of a multicenter Australian study. Surg. Neurol. Int. 2.
Falcioni, et al., 2018. Report of final results regarding brain and heart tumors in Sprague- Dawley rats exposed from prenatal life until natural death to mobile phone radiofrequency field representative of a 1.8 ghz gsm base station environmental emission. Environ. Res.
Fernandez-Rodriguez, C.E., De Salles, A.A.A., Davis, D.L., 2015. Dosimetric simulations of brain absorption of mobile phone radiation-the relationship between psSAR and age. IEEE Access 3, 2425–2430.
Frei, P., Poulsen, A.H., Johansen, C., Olsen, J.H., Steding-Jessen, M., Schüz, J., 2011. Use of mobile phones and risk of brain tumours: update of Danish cohort study. Br. Med. 343, d6387.
Genuis, S.J., Lipp, C.T., 2012. Electromagnetic hypersensitivity: fact or fiction? Sci. Total Environ. 414, 103–112. Gittleman, H.R., et al., 2015. Trends in central nervous system tumor incidence relative to other common cancers in adults, adolescents, and children in the United States, 2000 to 2010. Cancer 121 (1), 102–112.
Grell, K., et al., 2016. The intracranial distribution of gliomas in relation to exposure from mobile phones: analyses from the INTERPHONE study. Am. J. Epidemiol. 184 (11), 818–828.
Hardell, L., Carlberg, M., 2013. Using the Hill viewpoints from 1965 for evaluating strengths of evidence of the risk for brain tumors associated with use of mobile and cordless phones. Rev. Environ. Health 28, 97–106. https://doi.org/10.1515/reveh-2013-0006.
Hardell, L., Carlberg, M., 2015. Mobile phone and cordless phone use and the risk for glioma – analysis of pooled case-control studies in Sweden, 1997–2003 and 2007–2009. Pathophysiology 22 (1), 1–13.
Hardell, L., Carlberg, M., Mild, Kjell H., 2005. Use of cellular telephones and brain tumour risk in urban and rural areas. Occup. Environ. Med. 62 (6), 390–394.
Hardell, L., Carlberg, M., Söderqvist, F., Mild, Kjell H., 2013a. Pooled analysis of case-control studies on acoustic neuroma diagnosed 1997–2003 and 2007–2009 and use of mobile and cordless phones. Int. J. Oncol. 43 (4), 1036–1044.
Hardell, L., Carlberg, M., Söderqvist, F., Mild, Kjell H., 2013b. Case-control study of the association between malignant brain tumours diagnosed between 2007 and 2009 and mobile and cordless phone use. Int. J. Oncol. 43 (6), 1833–1845.
Houston, B.J., Nixon, B., King, B.V., De Iuliis, G.N., Aitken, R.J., 2016. The effects of radiofrequency electromagnetic radiation on sperm function. Reproduction 152, R263–R276.
IARC Monographs on the evaluation of carcinogenic risks to humans, 2013. Non-ionizing Radiation, Part 2: Radiofrequency Electromagnetic Fields 102 International Agency for Research on Cancer, Lyon.
INTERPHONE Study Group, 2010. Brain tumour risk in relation to mobile telephone use: results of the INTERPHONE international case-control study. Int. J. Epidemiol. 39 (3), 675–694.
Lehrer, S., Green, S., Stock, R.G., 2011. Association between number of cell phone contracts and brain tumor incidence in nineteen U.S. States. J. Neurooncology 101 (3), 505–507.
Kleijwegt, M., et al., 2016. Real Incidence of Vestibular Schwannoma? Estimations from a National Registry. Otol. Neurotol. 37 (9), 1411–1417.
Li, C.Y., et al., 2012. A population-based case-control study of radiofrequency exposure in relation to childhood neoplasm. Sci. Total Environ. 435–436, 472–478.
Markova, E., Malmgren, L.O.G., Belyaev, I.Y., 2010. Microwaves from mobile phones inhibit 53BP1 focus formation in human stem cells more strongly than in differentiated cells: possible mechanistic link to cancer risk. Environ. Health Perspect. 118 (3), 394–399.
McCarty, D.E., et al., 2011. Electromagnetic hypersensitivity: evidence for a novel neurological syndrome. Int. J. Neurosci. 121 (12), 670–676.
Momoli, F., et al., 2017. Probabilistic multiple-bias modeling applied to the canadian data from the interphone study of mobile phone use and risk of glioma, meningioma, acoustic neuroma, and parotid gland tumors. Am. J. Epidemiol. 186, 885–893. https://doi.org/10.1093/aje/kwx157.
Moon, I.S., et al., 2014. Association between vestibular schwannomas and mobile phone use. Tumor Biol. 35 (1), 581–587.
Morgan, L.L., Carlberg, M., 2010. Re-evaluation of the interphone study, application of a correction factor. Proceedings of the Bioelectromagnetics Society 32nd Annual Meeting Abstract Collection. June 14-18, pp. 391.
Morgan, L.L., Miller, A.B., Davis, D.L., 2016. Has the incidence of brain cancer risen in Australia since the introduction of mobile phones 29 years ago? Cancer Epidemiol. 44, 112–113.
National Toxicology Program, 2018a. NTP Technical Report on the Toxicolocy and Carcinogenesis Studies in Hsd:Sprague Dawley SD Rats Exposed to Whole-Body Radio Frequency Radiation at a Frequency (900 MHz) and Modulations (GSM and CDMA) Used by Cell Phones. NTP TR 595. 〈https://ntp.niehs.nih.gov/ntp/about_ntp/ trpanel/2018/march/tr595peerdraft.pdf〉.
National Toxicology Program, 2018b. NTP Technical Report on the Toxicolocy and Carcinogenesis Studies in B6C3F1/N Mice Exposed to Whole-Body Radio Frequency Radiation at a Frequency (1800 MHz) and Modulations (GSM and CDMA) Used by Cell Phones. NTP TR 596. 〈https://ntp.niehs.nih.gov/ntp/about_ntp/trpanel/2018/march/tr596peerdraft.pdf〉.
Navas-Acien, A., et al., 2002. Interactive effect of chemical substances and occupational electromagnetic field exposure on the risk of gliomas and meningiomas in Swedish men. Cancer Epidemiol., Biomark. Prev. 11, 1678–1683.
Prasad, M., et al., 2017. Mobile phone use and risk of brain tumours: a systematic review of association between study quality, source of funding, and research outcomes. Neurol. Sci. 38 (5), 797–810.
Peleg, M., 2009. Report on a cancer cluster in an antenna ranges facility. IEEE International Conference on Microwaves, Communications, Antennas and Electronics Systems (COMCAS),.
Peleg, M.A., 2012. Thermodynamic Perspective on the Interaction of Radio Frequency Radiation with Living Tissue. Int. J. Biophys. 2 (1), 1–6.
Peleg, M., Nativ, O., Richter, E.D., 2018. Radio frequency radiation-related cancer: assessing causation in the occupational/military setting. Environ. Res. 163, 123–133.
Pettersson, D., et al., 2014. Long-term mobile phone use and acoustic neuroma risk. Epidemiology 25 (2), 233–241.
Philips, A., Henshaw, D.L., Lamburn, G., O’Carroll, M.J., 2018. Brain tumours: rise in glioblastoma multiforme incidence in England 1995–2015 suggests an adverse environmental or lifestyle factor. J. Public Health Environ (in press).
Sadetzki, S., et al., 2014. The MOBI-Kids study protocol: challenges in assessing childhood and adolescent exposure to electromagnetic fields from wireless telecommunicationtechnologies and possible association with brain tumor risk. Front. Public Health 2 (124), 1–10.
Sato, Y., Kiyohara, K., Kojimahara, N., Yamaguchi, N., 2016. Time trend in incidence of malignant neoplasms of the central nervous system in relation to mobile phone use among young people in Japan. Bioelectromagnetics 37 (5), 282–289.
Sepehrimanesh, M., Kazemipour, N., Saeb, M., Nazifi, S., Davis, D.L., 2017. Proteomic analysis of continuous 900-MHz radiofrequency electromagnetic field exposure in testicular tissue: a rat model of human cell phone exposure. Environ. Sci. Pollut. Res Int 24 (15), 13666–13673. https://doi.org/10.1007/s11356-017-8882-z.
Stein, Y., Levy-Nativ, O., Richter, E.D., 2011. A sentinel case series of cancer patients with occupational exposures to electro-magnetic non-ionizing radiation and other agents. Eur. J. Oncol. 16, 21–54.
Szmigielski, S., 1996. Cancer morbidity in subjects occupationally exposed to high frequency (radiofrequency and microwave) electromagnetic radiation. Sci. Total Environ. 180, 9–17.
Tos, M., et al., 2004. What is the real incidence of vestibular schwannoma? Arch. Otolaryngol. Head. Neck Surg. 130 (2), 216–220.
West, J.G., et al., 2013. Multifocal breast cancer in young women with prolonged contact between their breasts and their cellular phones. Case Rep. Med (no. 354682).
Wojcik, D.P., 2016. Primary brain tumors and mobile cell phone usage. Cancer Epidemiol. 44 (2016), 123–124.
www.CBTRUS.org. Reports and Tables (Accessed 14 May 2016).
Yang, M., et al., 2017. Mobile phone use and glioma risk: a systematic review and metaanalysis. PLoS ONE 12 (5).
Zada, G., et al., 2012. Incidence trends in the anatomic location of primary malignant brain tumors in the United States: 1992–2006. World Neurosurg. 77 (3–4), 518–524.
Miller, A. B. et al. (2018).Cancer epidemiology update, following the 2011 IARC evaluation of radiofrequency electromagnetic fields (Monograph 102). Environmental Research, doi: 10.1016/j.envres.2018.06.043[